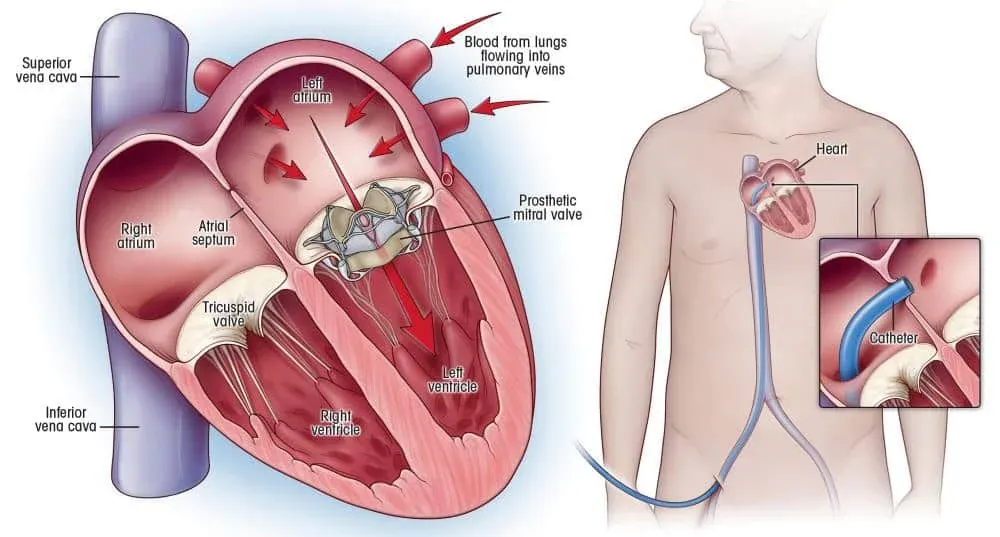
በህንድ ውስጥ የልብ ቫልቭ ምትክ ቀዶ ጥገና፡ ዓይነቶች፣ ቴክኖሎጂዎች እና መልሶ ማግኛ
ተዛማጅ ሆስፒታሎች
ጥራት ያለው የጤና እንክብካቤ አገልግሎቶች ከዚህ ርዕስ ጋር የሚዛመዱ ሆስፒታሎች እና የህክምና ማዕከሎች ያግኙ.

የሕክምና ፓርክ Bahcelievler ሆስፒታል
ሜዲካል ፓርክ Bahcelievler ሆስፒታል በ 242 አልጋ JCI እውቅና ያለው በኢስታንቡል ውስጥ የሚገኝ ሆስፒታል ነው በ2007 የተቋቋመ። ሆስፒታሉ ኤምአርአይ፣ ሲቲ እና አንጂዮግራፊን ጨምሮ 10 የቀዶ ሕክምና ክፍሎች፣ 89 የተመላላሽ...
መድኃኒቶች

መገልገያዎች

BLK-ማክስ ሱፐር ስፔሻሊቲ ሆስፒታል፣ ኒው ዴሊ
በኒው ዴሊ የሚገኘው BLK-Max Super Specialty ሆስፒታል 650 አልጋዎች፣ 22 የላቁ የኦፕሬሽን ቲያትሮች እና 13 የልህቀት ማእከላት በማቅረብ ከህንድ የመጀመሪያ የጤና እንክብካቤ ተቋማት አንዱ ነው። በአለም አቀፍ ደረጃ በካን...
መድኃኒቶች

መገልገያዎች

Fortis Memorial Research Institute (FMRI), Gurgaon
Fortis Memorial Research Institute (FMRI) Gurgaon በ 2013 የተቋቋመ አለም አቀፍ ደረጃውን የጠበቀ የብዝሃ-ስፔሻሊቲ ሆስፒታል ነው። ሆስፒታሉ 330 አልጋዎች፣ 15 የቀዶ ህክምና ቲያትሮች፣ 105 አይሲዩ አል...
መድኃኒቶች
መገልገያዎች

አርጤምስ ሆስፒታል ፣ ጉራጌን።
Artemis Hospital, Gurgaon በ 2007 የተቋቋመ JCI እውቅና ያለው ሁለገብ ልዩ ሆስፒታል ነው። 750+ አልጋዎች እና በ9 ሄክታር ላይ የሚሰራጩ አለም አቀፍ ደረጃ መሠረተ ልማቶችን ያቀርባል። አርጤምስ M6 CyberKnife...
መድኃኒቶች

መገልገያዎች

ኮኪላበን ድሩብሃይ አምባኒ ሆስፒታል፣ ሙምባይ
Kokilaben Dhirubhai Ambani ሆስፒታል፣ ሙምባይ፣ በJCI፣ NABH፣ NABL እና CAP እውቅና ያለው የኳተርን እንክብካቤ ሆስፒታል በ2009 የተቋቋመ ነው። በ750 አልጋዎች፣ 180 ICU አልጋዎች እና 22 የላቁ የኦፕሬሽን...
መድኃኒቶች
መገልገያዎች

Medicover ሆስፒታሎች፣ Hitech City፣ Hyderabad
ሜዲኮቨር ሆስፒታሎች፣ ሂቴክ ሲቲ፣ ሃይደራባድ፣ በ 2011 በ 400 አልጋ በ NABH እውቅና ያለው ሱፐር-ስፔሻሊቲ ሆስፒታል የተቋቋመ ነው። በ18 አገሮች ውስጥ የሚሰራው የሜዲኮቭር፣ አለም አቀፍ እውቅና ያለው የጤና እንክብካቤ ብራንድ አ...
መድኃኒቶች
መገልገያዎች
ተዛማጅ ሐኪሞች
በዚህ መስክ ውስጥ ካሉ ልምዶች ተሞክሮዎች እና የሕክምና ባለሞያዎች ጋር ይገናኙ.

ዶክተር Kaushik Mukherjee
አማካሪ

ዶክተር ሱፐራቲፕ ኩንዱ
አማካሪ

ዶክተር ሱማን ሃልደር
ጉብኝት አማካሪ

ዶክተር ሞኖቶሽ ፓንጃ
ከፍተኛ አማካሪ

ዶክተር ሄማ ማላቲ ራት
ከፍተኛ አማካሪ

ዶ/ር ኢምራን አህመድ
ከፍተኛ አማካሪ
ተዛማጅ መጣጥፎች
ተመሳሳይ የጤና ርዕሶችን በተመለከተ ተጨማሪ ርዕሶችን እና ግንዛቤዎችን ያስሱ.

ህንድ ከታይላንድ፡ በ2026 ምርጡ የህክምና ቱሪዝም መድረሻ የትኛው ነው?

በህንድ ውስጥ ሮቦቲክ ፕሮስቴትቶሚ: ነርቭ-የማዳን ዘዴዎች, ማገገም እና የታካሚ ውጤቶች
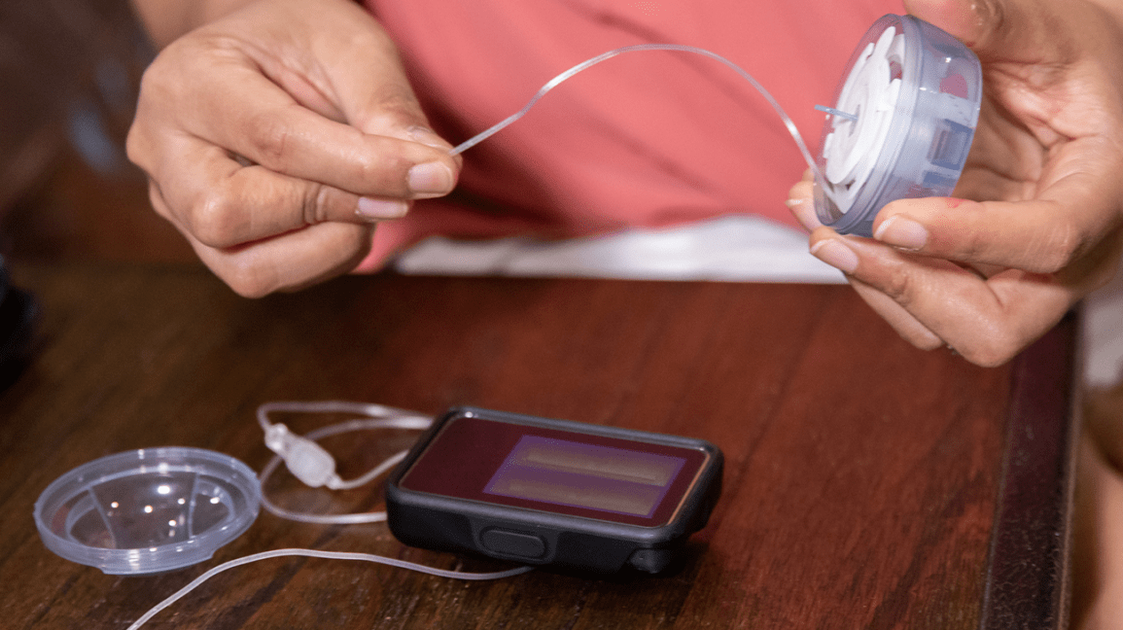
የኢንሱሊን ፓምፕ ሕክምና፡ እንዴት እንደሚሰራ፣ ማን እንደሚጠቅመው እና በ2026 ምን እንደሚያስከፍል

ከመጠን ያለፈ ውፍረት እና የስኳር በሽታ፡- የባሪያት ቀዶ ጥገና ሁለቱንም በአንድ ላይ እንዴት እንደሚፈታ
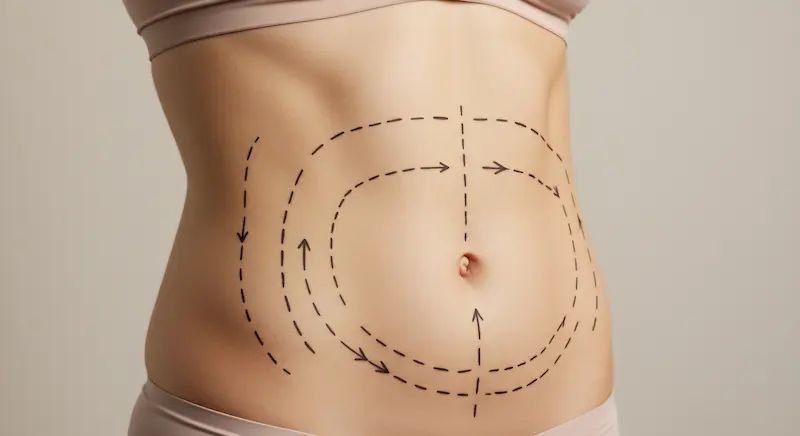
Liposuction በህንድ ውስጥ፡ ቴክኒኮች፣ ወጪዎች እና የማገገሚያ ጊዜ

የፊት ላይፍ ቀዶ ጥገና በህንድ፡ ሂደት፣ ማገገም እና ምርጥ የቀዶ ጥገና ሐኪሞችን መምረጥ

ድር ጣቢያችን ኩኪዎችን ይጠቀማል. የግላዊነት ፖሊሲ.