Robotic Prostatectomy in India: Nerve-Sparing Techniques, Recovery, and Patient Outcomes

Əlaqəli xəstəxanalar
Keyfiyyətli sağlamlıq xidmətləri üçün bu mövzu ilə əlaqəli xəstəxanalar və tibb mərkəzlərini kəşf edin.

Medical Park Bahçelievler Xəstəxanası
Medical Park Bahçelievler Xəstəxanası İstanbulda 2007-ci ildə qurulmuş 242 çarpayılıq JCI tərəfindən akkreditə olunmuş xəstəxanadır. 33.000 kvadratmet...
Akkreditasiyalar

Qurğu

BLK-Max Super İxtisas Xəstəxanası, Yeni Dehli
Yeni Dehlidəki BLK-Max Super İxtisas Xəstəxanası 650 çarpayı, 22 qabaqcıl əməliyyat teatrı və 13 Mükəmməllik Mərkəzi təklif edən Hindistanın ən yaxşı ...
Akkreditasiyalar

Qurğu

Fortis Memorial Tədqiqat İnstitutu (FMRI), Gurgaon
Fortis Memorial Araşdırma İnstitutu (FMRI), Gurgaon, 2013-cü ildə yaradılmış dünya səviyyəli çoxixtisaslı xəstəxanadır. Xəstəxana 330 çarpayı, 15 əməl...
Akkreditasiyalar
Qurğu

Artemis Xəstəxanası, Gurgaon
Artemis Xəstəxanası, Gurqaon, 2007-ci ildə yaradılmış JCI tərəfindən akkreditə olunmuş çoxixtisaslı xəstəxanadır. O, 9 hektar əraziyə yayılmış 750+ ça...
Akkreditasiyalar

Qurğu

Kokilaben Dhirubhai Ambani Xəstəxanası, Mumbay
Kokilaben Dhirubhai Ambani Xəstəxanası, Mumbay, 2009-cu ildə yaradılmış JCI, NABH, NABL və CAP tərəfindən akkreditə olunmuş dördüncü dərəcəli baxım xə...
Akkreditasiyalar
Qurğu

Medicover Xəstəxanaları, Hitech City, Hyderabad
Medicover Hospitals, Hitech City, Hyderabad, is a 400-bed NABH-accredited super-specialty hospital established in 2011. It is part of Medicover, a glo...
Akkreditasiyalar
Qurğu
Oxşar həkimlər
Bu sahədə təcrübəli həkimlər və tibbi mütəxəssislərlə əlaqə qurun.
Dr. Bibhas Ranjan Kundu
Baş Məsləhətçi
Dr. Revathi R
məsləhətçi

Dr. Prasad Raju Kalidindi
Baş Məsləhətçi
Dr. Şakir Təbriz
Əlavə Direktor
Dr. Wichean Kamolpornvijit
məsləhətçi

Dr. Ukrid Kesthong
məsləhətçi
Əlaqədar məqalələr
Bənzər sağlamlıq mövzularında daha çox məqalə və anlayışları araşdırın.

Hindistan vs Tayland: 2026-cı ildə ən yaxşı tibbi turizm yeri hansıdır?
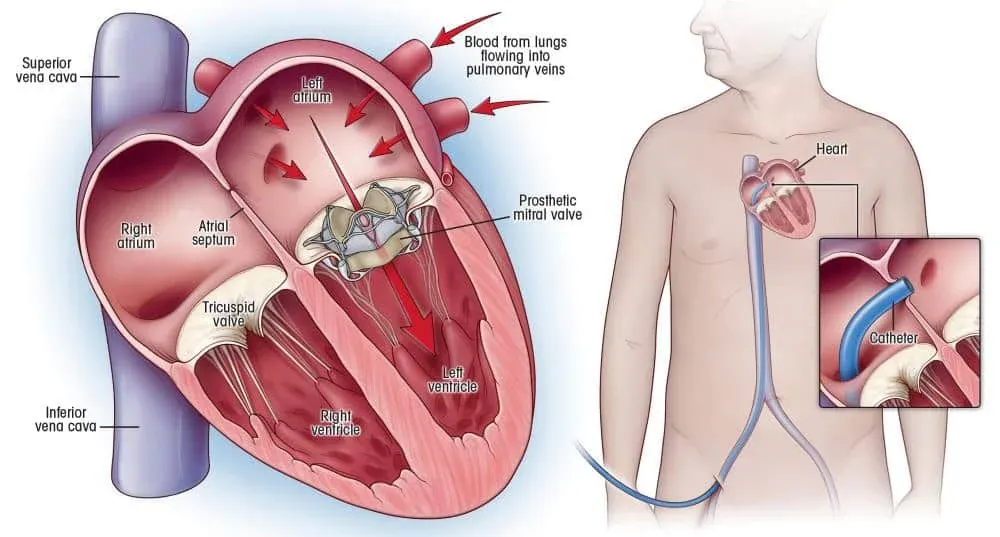
Hindistanda ürək qapaqlarının dəyişdirilməsi əməliyyatı: növləri, texnologiyaları və bərpası
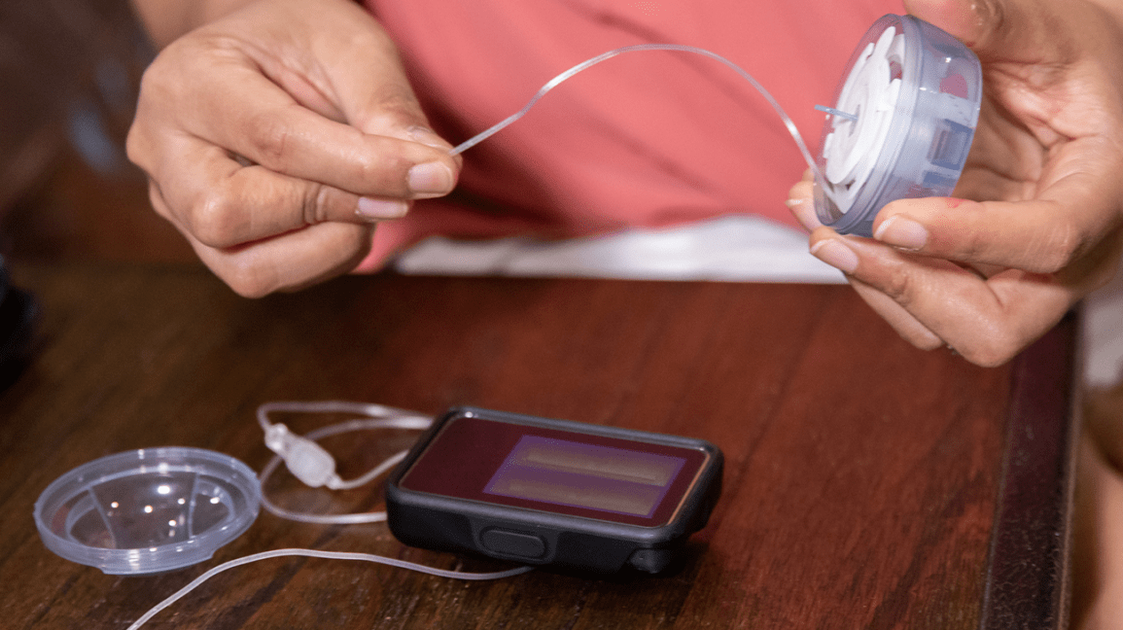
İnsulin nasos terapiyası: necə işləyir, kimə fayda verir və 2026-cı ildə nəyə başa gəlir

Piylənmə və Diabet: Bariatrik Cərrahiyyə hər ikisini birlikdə necə həll edir
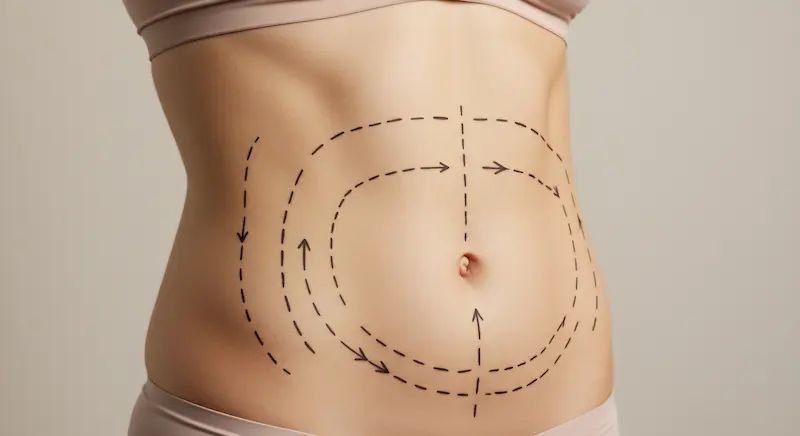
Hindistanda Liposuction: Texnikalar, Xərclər və Bərpa Xronologiyası

Hindistanda Facelift Cərrahiyyə: Prosedur, Bərpa və Ən Yaxşı Cərrahların Seçilməsi

Veb saytımız çərəzlərdən istifadə edir. Məxfilik Siyasəti.