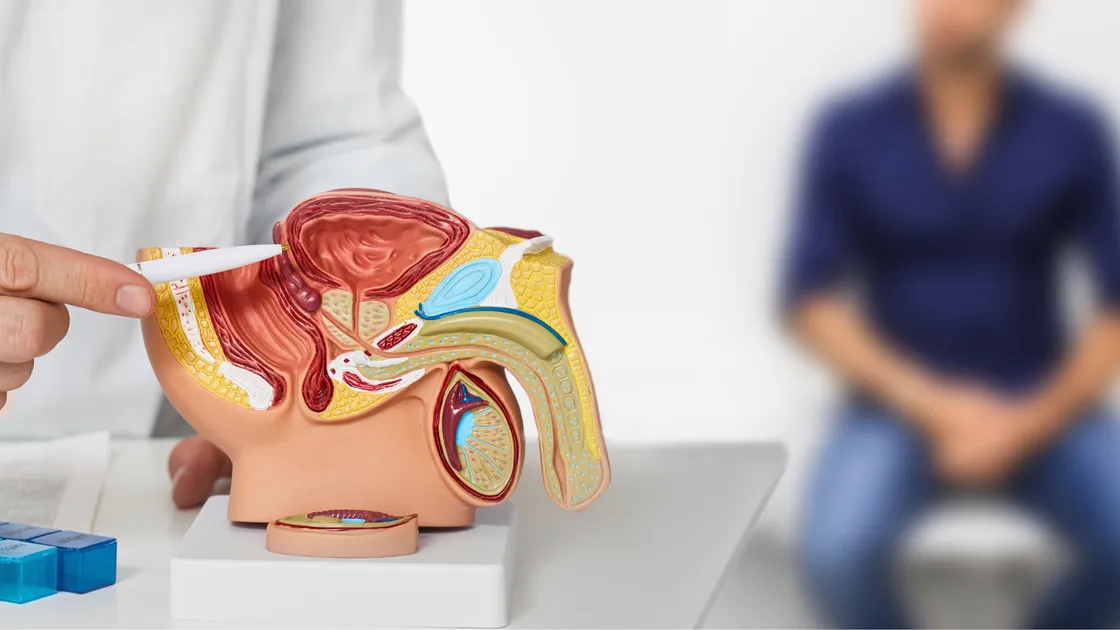
HoLEP vs TURP ee Prostate-ka Weyn: Nidaamkee Ayaa Wanagsan?
Isbitaalada la xiriira
Baro Isbitaalada iyo xarumaha caafimaadka ee la xiriira mowduucan adeegyada daryeelka caafimaadka tayada leh.

Park Medical Bahcelievler Hospital
Medical Park Bahcelievler Hospital waa cisbitaal la aqoonsan yahay JCI oo leh 242 sariirood oo ku yaal Istanbul, oo la aasaasay 2007. Ku faafaya 33,00...
Aqoonsado

Gadawiya xarumaha

BLK-Max Super Specialty Hospital, New Delhi
BLK-Max Super Specialty Hospital ee New Delhi waa mid ka mid ah xarumaha daryeelka caafimaadka ee Hindiya, oo bixiya 650 sariirood, 22 tiyaatar qallii...
Aqoonsado

Gadawiya xarumaha

Fortis Memorial Research Institute (FMRI), Gurgaon
Fortis Memorial Research Institute (FMRI), Gurgaon, waa isbitaal heer caalami ah oo badan oo takhasus leh oo la aasaasay 2013. Isbitaalku wuxuu bixiya...
Aqoonsado
Gadawiya xarumaha

Isbitaalka Artemis, Gurgaon
Cisbitaalka Artemis, Gurgaon, waa cisbitaalka takhasuska badan ee JCI la aqoonsan yahay oo la aasaasay 2007. Waxa uu bixiyaa 750+ sariirood iyo kaabay...
Aqoonsado

Gadawiya xarumaha

Isbitaalka Kokilaben Dhirubhai Ambani, Mumbai
Kokilaben Dhirubhai Ambani Hospital, Mumbai, waa JCI, NABH, NABL, iyo CAP-la aqoonsan cusbitaalka daryeelka afargeesoodka ah oo la aasaasay 2009. Iyad...
Aqoonsado
Gadawiya xarumaha

Isbitaalada Medicover, Hitech City, Hyderabad
Isbitaalada Medicover, Hitech City, Hyderabad, waa 400-sariirood oo NABH ah oo la aqoonsan yahay cosbitaal sare oo gaar ah oo la aasaasay 2011. Waa qa...
Aqoonsado
Gadawiya xarumaha
Dhakhaatiirta la xiriira
Ku xir dhakhaatiir khibrad leh iyo khabiiro caafimaad oo arimahan ah.
Dr. Bibhas Ranjan Kundu
La-taliye sare
Dr. Revathi R
La-taliye

Dr. Prasad Raju Kalidindi
La-taliye sare
Dr. Shaakir Tabrez
Agaasime dheeraad ah
Dr. Wichean Kamolportnvijit
La-taliye

Dr. Ukrid Kesthong
La-taliye
Maqaallada la xiriira
Sahamiyaan maqaallo badan iyo aragtiyo ku saabsan mowduucyada caafimaadka ee la midka ah.
PCNL vs ESWL ee Dhagxaanta Kelyaha: keebaa Wanagsan iyo Goorma?
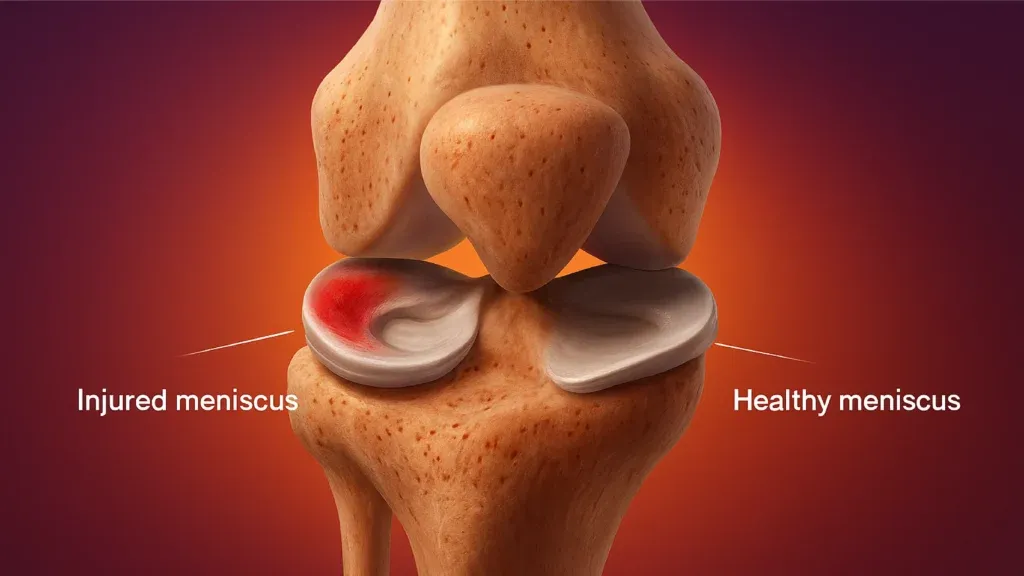
Dayactirka MCL iyo Meniscus ee Hindiya: Qalliinka, Heerka Guusha, iyo Soo kabashada

Rotator Cuff Repair Surgery in India: Procedure, Success Rates and Cost
Best Countries for Orthopaedic Surgery and Sports Medicine in 2026
Qalliinka Dib-u-dhiska ACL ee Hindiya: Habka, Qiimaha, iyo Heerka Guusha
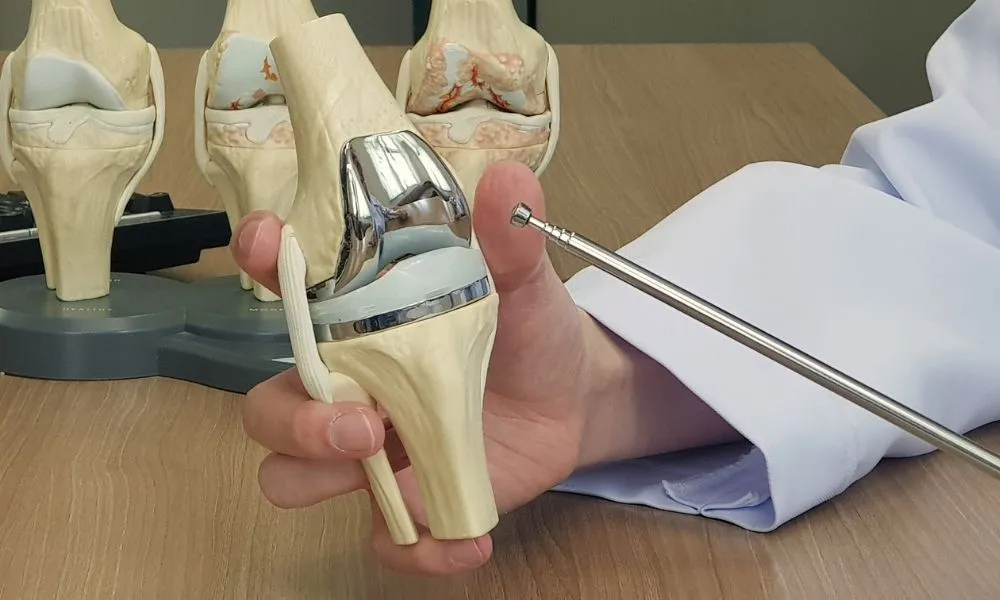
Beddelka garabka ee Hindiya: Qiimaha, Habka, Soo kabashada

Websaydhkeenu wuxuu adeegsadaa cookies. Qaanuunka Arrimaha Khaaska ah.