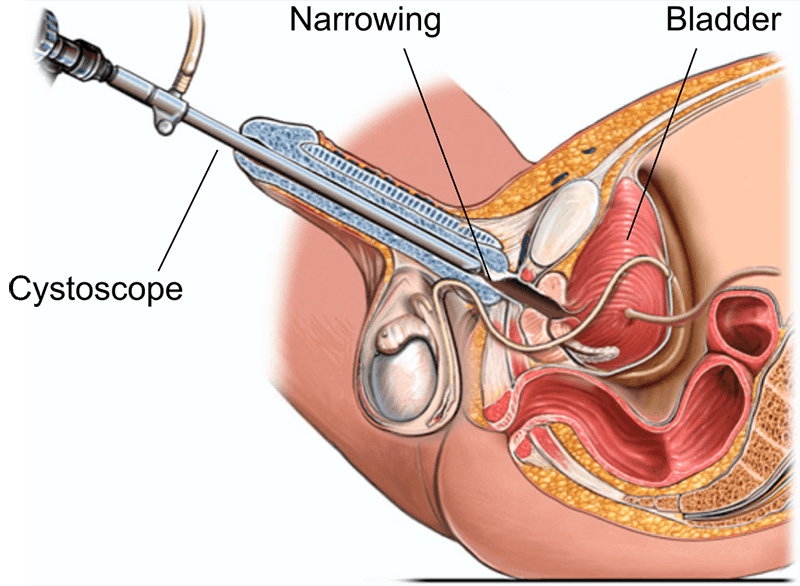
Hindistanda peşew çykaryş usuly: prosedura, üstünlik derejeleri, çykdajylar we dikeldiş
Baglanyşykly hassahanalar
Hil saglygy goraýyş hyzmatlary üçin bu mowzugy bilen hassahanalary we lukmançylyk merkezlerini öwreniň.

Lukmançylyk seýilgähi Bahçeliýewler hassahanasy
Medisina Park Bahçeliýewler hassahanasy, 2007-nji ýylda döredilen Stambulda 242 orunlyk JCI akkreditlenen hassahanadyr. 33,000 inedördül metr we 19 ga...
Akkreditasiýa

Desgalar

“BLK-Max” ýörite hünär hassahanasy, Nýu-Deli
Nýu-Delidäki “BLK-Max Super” ýörite hassahanasy 650 krowat, 22 sany öňdebaryjy operasiýa teatry we 13 sany ajaýyp merkez hödürleýän Hindistanda iň esa...
Akkreditasiýa

Desgalar

Fortis Memorial gözleg instituty (FMRI), Gurgaon
Gurgaon şäherindäki Fortis Memorial gözleg instituty (FMRI) 2013-nji ýylda döredilen dünýä derejesindäki köp hünärli hassahanadyr. Keselhana 330 krowa...
Akkreditasiýa
Desgalar

Artemis hassahanasy, Gurgaon
Gurgaon, Artemis hassahanasy, 2007-nji ýylda döredilen JCI akkreditlenen köp hünärli hassahanadyr. 9 gektar meýdanda 750+ düşek we dünýä derejesindäki...
Akkreditasiýa

Desgalar

Kokilaben Dhirubhai Ambani hassahanasy, Mumbay
Mumbay, Kokilaben Dhirubhai Ambani hassahanasy, 2009-njy ýylda döredilen JCI, NABH, NABL we CAP tarapyndan akkreditlenen dört taraplaýyn bejeriş hassa...
Akkreditasiýa
Desgalar

Medicover hassahanalary, Hitech şäheri, Haýdarabat
Medicover hassahanalary, Haýdarabadyň Hitech şäheri, 2011-nji ýylda döredilen 400 orunlyk NABH akkreditlenen super ýöriteleşdirilen hassahanadyr. 18 ý...
Akkreditasiýa
Desgalar
Baglanyşykly lukmanlar
Bu ugurda tejribeli lukmanlar we lukmançylyk hünärmenleri bilen birikdiriň.
Dr. Bibhas Ranjan Kundu
Uly geňeşçi
Dr. Revathi R.
Maslahatçy

Dr. Prasad Raju Kalidindi
Uly geňeşçi
Dr. Şakir Tabrez
Goşmaça direktor
Dr. Wichean Kamolpornvijit
Maslahatçy

Dr. Ukrid Kesthong
Maslahatçy
Degişli makalalar
Şuňa meňzeş saglyk temalarynda has köp makalalary we düşünjeleri öwreniň.
Böwrek daşlary üçin PCNL vs ESWL: Haýsy gowy we haçan?
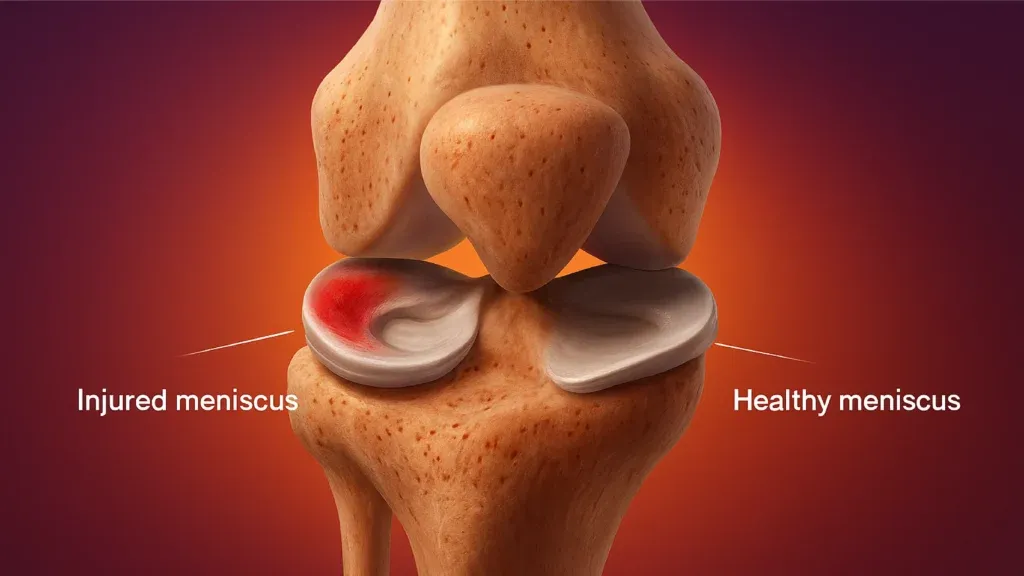
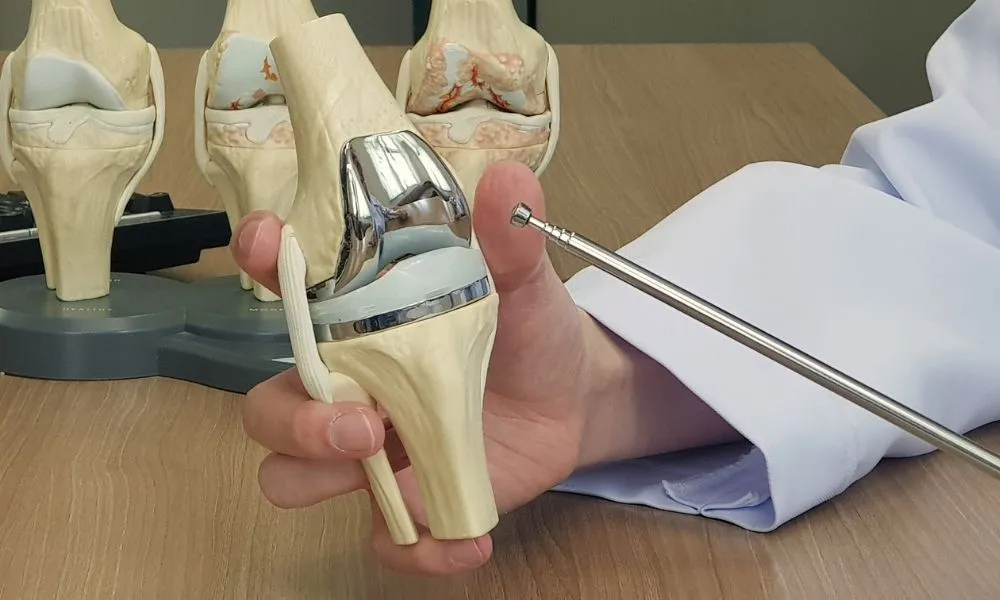
Hindistanda MCL we Meniskus bejergisi: hirurgiýa, üstünlik derejesi we dikeldiş

Rotator Cuff Repair Surgery in India: Procedure, Success Rates and Cost
Best Countries for Orthopaedic Surgery and Sports Medicine in 2026
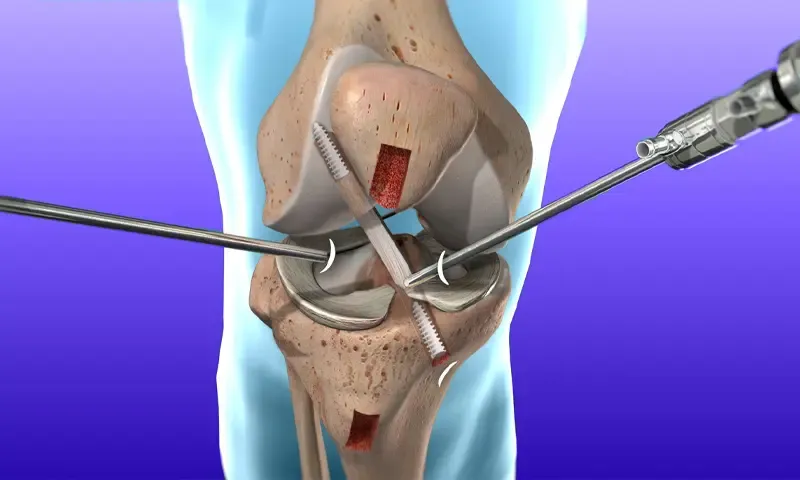
Hindistanda ACL rekonstruksiýa hirurgiýasy: tertibi, bahasy we üstünlik derejesi
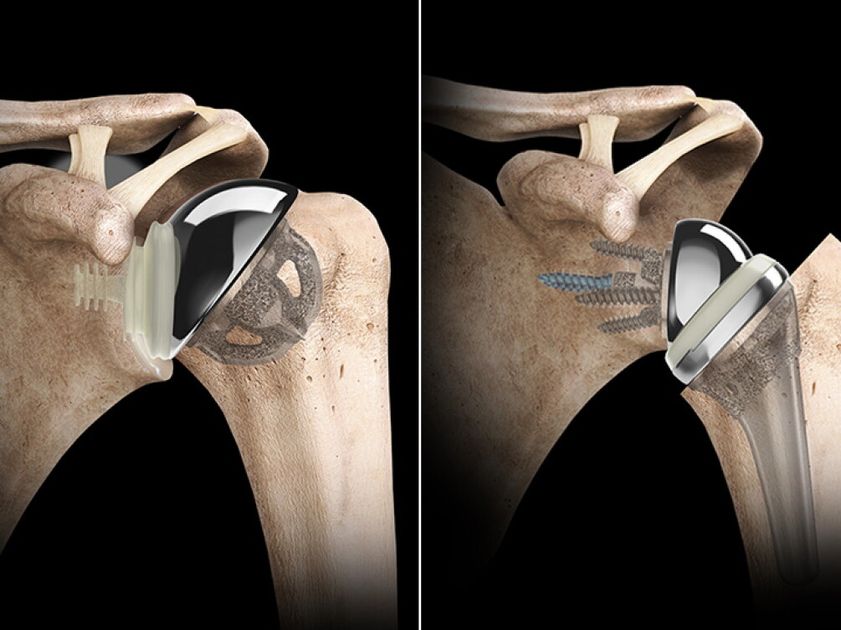
Hindistanda tersi egin çalyşmak: Bahasy, tertibi, dikeldişi

Sahypamyz gutapjyk ulanýar. Gizlinlik syýasaty.