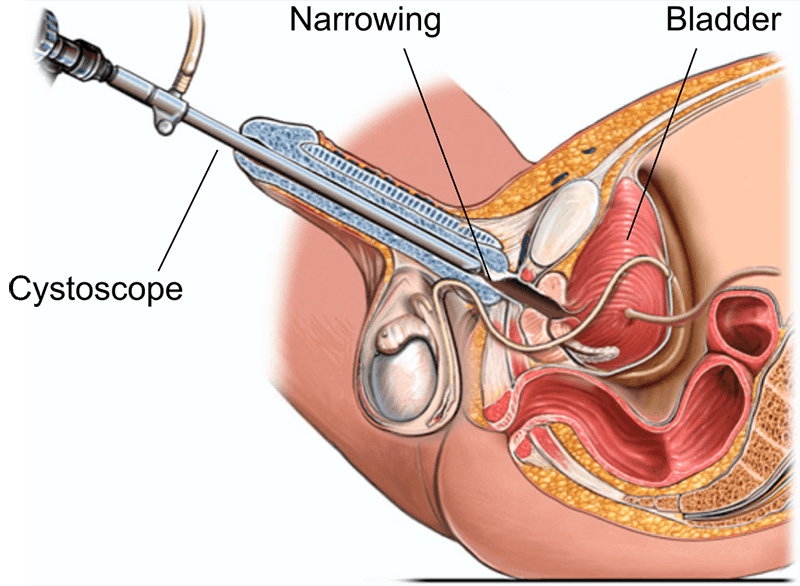
Индияда уретропластика: жол-жобосу, ийгилик курстары, наркы жана калыбына келтирүү
Тиешелүү ооруканалар
Сапаттуу медициналык кызматтар үчүн ушул темага байланышкан ооруканаларды жана медициналык борборлорду таап алыңыз.

Medical Park Bahcelievler ооруканасы
Medical Park Bahcelievler ооруканасы 2007-жылы негизделген Стамбулдагы 242 койкалуу JCI тарабынан аккредиттелген оорукана. 33 000 чарчы метр жана 19 к...
Аккредитациялар

Жайлар

BLK-Max Супер адистештирилген ооруканасы, Нью-Дели
Нью-Делидеги BLK-Max Super Specialty Hospital Индиянын эң алдыңкы саламаттыкты сактоо мекемелеринин бири, 650 керебетти, 22 өркүндөтүлгөн операциялык ...
Аккредитациялар

Жайлар

Fortis Memorial изилдөө институту (FMRI), Гургаон
Fortis Memorial изилдөө институту (FMRI), Гургаон, 2013-жылы түзүлгөн дүйнөлүк класстагы көп адистештирилген оорукана болуп саналат. Оорукана 330 кере...
Аккредитациялар
Жайлар

Артемис ооруканасы, Гургаон
Артемис ооруканасы, Гургаон, 2007-жылы түзүлгөн JCI аккредитацияланган көп адистиктеги оорукана. Ал 9 акр жерге жайылган 750+ керебетти жана дүйнөлүк ...
Аккредитациялар

Жайлар

Кокилабен Дирубхай Амбани ооруканасы, Мумбай
Кокилабен Дирубхай Амбани ооруканасы, Мумбай, 2009-жылы түзүлгөн JCI, NABH, NABL жана CAP тарабынан аккредиттелген төртүнчү медициналык оорукана. 750 ...
Аккредитациялар
Жайлар

Медиковер ооруканалары, Хитех шаары, Хайдарабад
Medicover Hospitals, Hitech City, Хайдарабад, 2011-жылы түзүлгөн 400 койкалуу NABH тарабынан аккредиттелген супер адистештирилген оорукана. Ал Medicov...
Аккредитациялар
Жайлар
Related Doctors
Тажрыйбалуу дарыгерлер жана медициналык адистер менен байланышыңыз.
Доктор Бибхас Ранжан Кунду
Улук консультант
Доктор Ревати Р
Консультант

Доктор Прасад Раджу Калидинди
Улук консультант
Доктор Шакир Табрез
Кошумча директор
Доктор Вичеан Камолпорнвижит
Консультант

Доктор Укрид Кестхонг
Консультант
Тектеш макалалар
Саламаттыкты сактоо темаларында көбүрөөк макалаларды жана түшүнүктөрдү изилдөө.
Бөйрөктөгү таштар үчүн PCNL vs ESWL: кайсынысы жакшы жана качан?
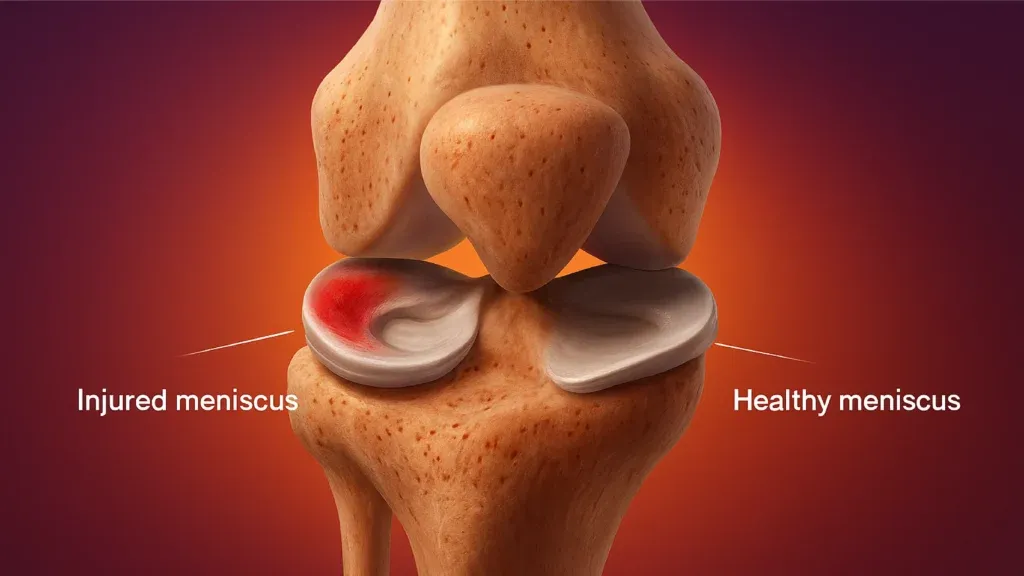
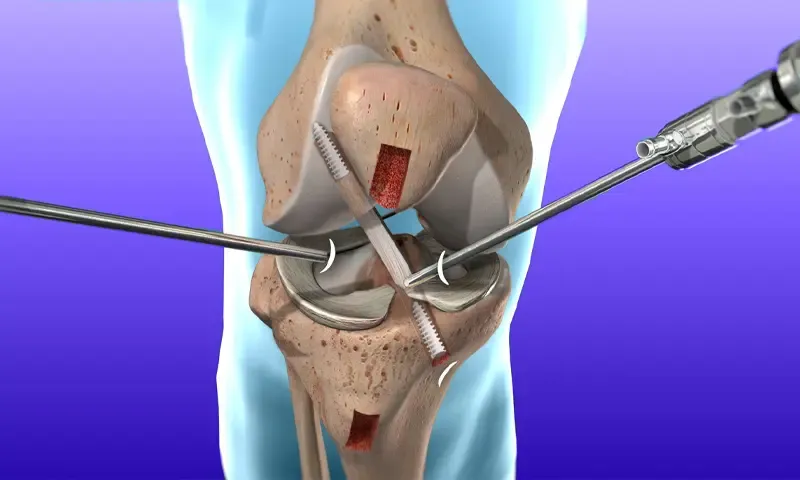
Индияда MCL жана Meniscus оңдоо: хирургия, ийгилик курсу жана калыбына келтирүү

Rotator Cuff Repair Surgery in India: Procedure, Success Rates and Cost
Best Countries for Orthopaedic Surgery and Sports Medicine in 2026
Индияда ACL калыбына келтирүү хирургиясы: тартиби, наркы жана ийгилик курсу
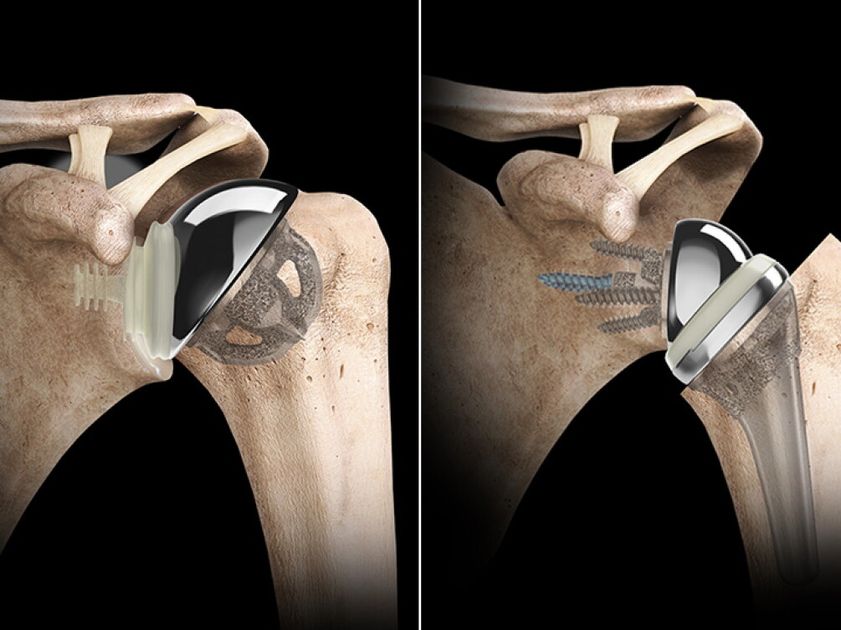
Индияда тескери ийин алмаштыруу: наркы, тартиби, калыбына келтирүү

Биздин веб-сайтта кукилерди колдонот. Купуялык саясаты.