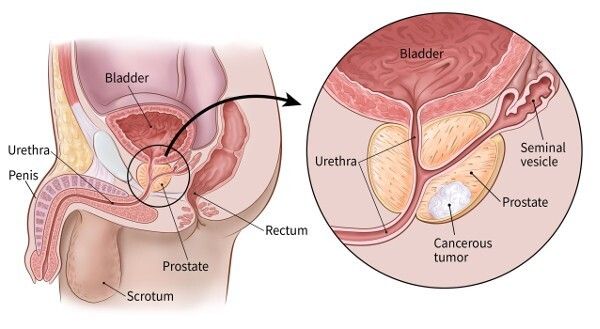
Robotic Prostatectomy in India: Nerve-Sparing Techniques, Recovery, and Patient Outcomes

Relaterade sjukhus
Upptäck sjukhus och vårdcentraler med anknytning till detta ämne för kvalitetssjukvård.

Medical Park Bahcelievler Hospital
Medical Park Bahcelievler Hospital är ett JCI-ackrediterat sjukhus med 242 bäddar i Istanbul, etablerat 2007. Den är spridd över 33 000 kvadratmeter o...
Ackrediteringar

Faciliteter

BLK-Max Super Specialty Hospital, New Delhi
BLK-Max Super Specialty Hospital i New Delhi är en av Indiens främsta vårdinstitutioner, som erbjuder 650 bäddar, 22 avancerade operationssalar och 13...
Ackrediteringar

Faciliteter

Fortis Memorial Research Institute (FMRI), Gurgaon
Fortis Memorial Research Institute (FMRI), Gurgaon, är ett multispecialitetssjukhus i världsklass som etablerades 2013. Sjukhuset erbjuder 330 bäddar,...
Ackrediteringar
Faciliteter

Artemis Hospital, Gurgaon
Artemis Hospital, Gurgaon, is a JCI accredited multispecialty hospital that was established in 2007. It offers 750+ beds and world -class infrastructu...
Ackrediteringar

Faciliteter

Kokilaben Dhirubhai Ambani Hospital, Mumbai
Kokilaben Dhirubhai Ambani Hospital, Mumbai, är ett JCI-, NABH-, NABL- och CAP-ackrediterat sjukhus för kvartärvård etablerat 2009. Med 750 bäddar, 18...
Ackrediteringar
Faciliteter

Medicover sjukhus, Hitech City, Hyderabad
Medicover Hospitals, Hitech City, Hyderabad, är ett NABH-ackrediterat superspecialitetssjukhus med 400 bäddar som grundades 2011. Det är en del av Med...
Ackrediteringar
Faciliteter
Besläktade läkare
Ta kontakt med erfarna läkare och medicinska specialister inom detta område.
Dr Bibhas Ranjan Kundu
senior konsult
Dr Revathi R
konsulterande läkare

Dr Prasad Raju Kalidindi
senior konsult
Dr Shakir Tabrez
extrachef
Dr Wichean Kamolpornvijit
konsulterande läkare

Dr Ukrid Kesthong
konsulterande läkare
Relaterade artiklar
Utforska fler artiklar och insikter om liknande hälsoämnen.
HIFU-behandling för prostatacancer i Indien: procedur, kostnad och återhämtning

Laserlitotripsi i Indien: procedur, teknik, kostnad och återhämtning

Är min sjukförsäkring giltig i Indien? En guide för internationella patienter

Indien vs Thailand: Vilket är det bästa medicinska turistmålet 2026?
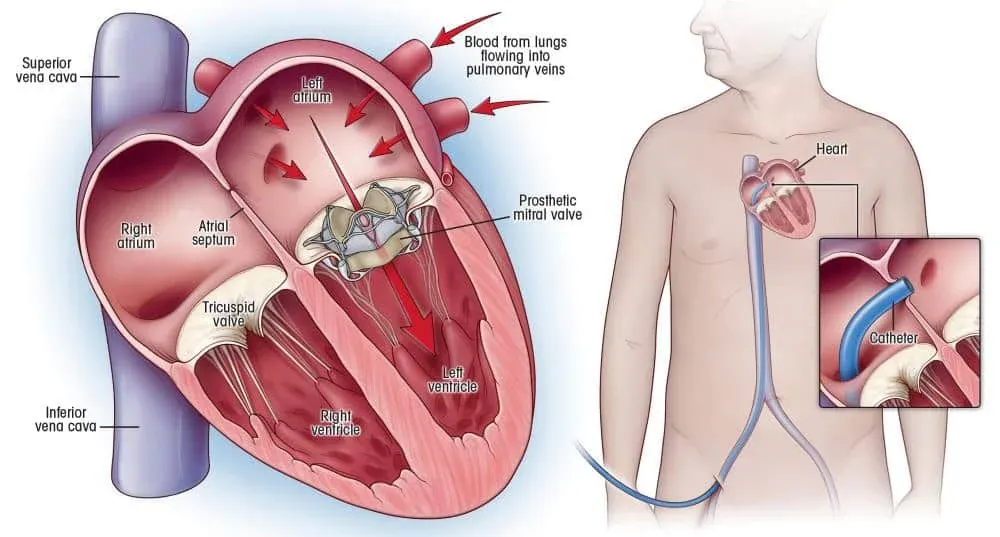
Hjärtklaffsersättningskirurgi i Indien: typer, teknologier och återhämtning
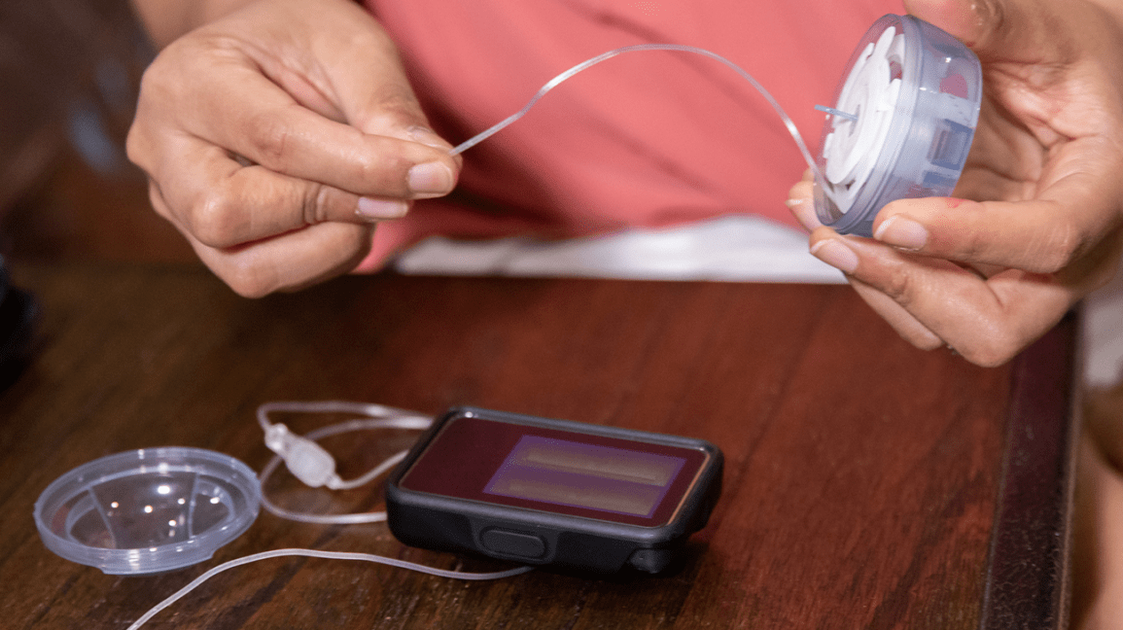
Insulinpumpsterapi: Hur det fungerar, vem som tjänar på det och vad det kostar 2026

Vår webbplats använder cookies. Sekretesspolicy.