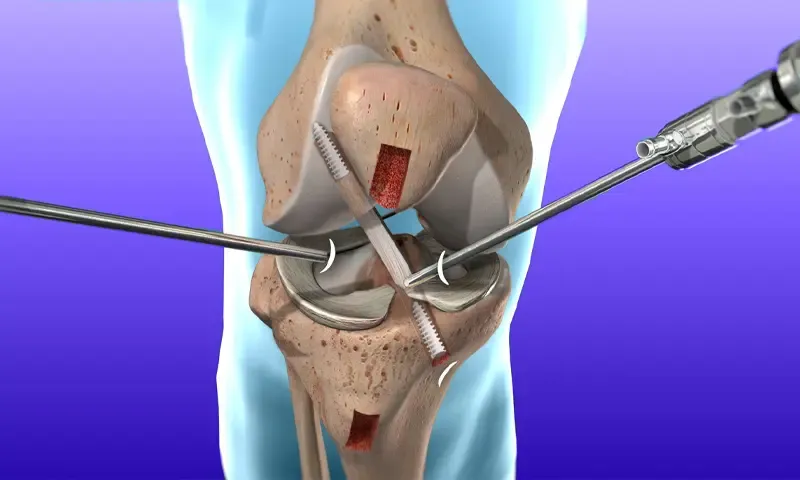
Hindistonda ACL rekonstruksiya jarrohligi: protsedura, narx va muvaffaqiyat darajasi
Tegishli kasalxonalar
Sifatli tibbiy xizmatlar uchun ushbu mavzu bilan bog'liq kasalxonalar va tibbiyot markazlarini kashf eting.

Medical Park Bahcelievler kasalxonasi
Medical Park Baxchelievler kasalxonasi 2007-yilda tashkil etilgan Istanbuldagi 242 oʻrinli JCI akkreditatsiyadan oʻtgan shifoxona boʻlib. 33 000 kvadr...
Akkreditatsiya

Muvofiqliklar

BLK-Max super ixtisoslashtirilgan kasalxonasi, Nyu-Dehli
Nyu-Dehlidagi BLK-Max Super Specialty Hospital 650 o'rinli yotoq, 22 ta ilg'or operasiya teatri va 13 ta mukammallik markazlarini taklif qiluvchi Hind...
Akkreditatsiya

Muvofiqliklar

Fortis Memorial tadqiqot instituti (FMRI), Gurgaon
Fortis Memorial Research Institute (FMRI), Gurgaon, 2013-yilda tashkil etilgan jahon miqyosidagi ko‘p ixtisoslashgan shifoxonadir. Kasalxona 330 ta yo...
Akkreditatsiya
Muvofiqliklar

Artemis kasalxonasi, Gurgaon
Artemis kasalxonasi, Gurgaon, 2007-yilda tashkil etilgan JCI akkreditatsiyadan oʻtgan koʻp ixtisoslashgan shifoxonadir. U 9 akr maydonda 750+ oʻrinli ...
Akkreditatsiya

Muvofiqliklar

Kokilaben Dhirubhai Ambani kasalxonasi, Mumbay
Kokilaben Dhirubhai Ambani kasalxonasi, Mumbay, 2009-yilda tashkil etilgan JCI, NABH, NABL va CAP tomonidan akkreditatsiya qilingan toʻrtlamchi tibbiy...
Akkreditatsiya
Muvofiqliklar

Medicover kasalxonalari, Hitech Siti, Haydarobod
Medicover Hospitals, Hitech City, Haydarobod, 2011-yilda tashkil etilgan 400 oʻrinli NABH akkreditatsiyasidan oʻtgan oʻta ixtisoslashgan shifoxonadir....
Akkreditatsiya
Muvofiqliklar
Tegishli shifokorlar
Ushbu sohada tajribali shifokorlar va tibbiyot mutaxassislari bilan bog'laning.

Doktor Kanchan Bhattacharyya
Maslahatchi

Doktor Kalyan Guha
Maslahatchi

Doktor Rajinder Singx Gahir
Katta maslahatchi

Dr. Ravi Bharadwaj
Katta maslahatchi

Doktor Ranjan Komilya
Katta maslahatchi

Doktor Abheek Kar
Maslahatchi
Tegishli maqolalar
Shunga o'xshash sog'liqni saqlash mavzularida boshqa maqolalar va tushunchalarni o'rganing.
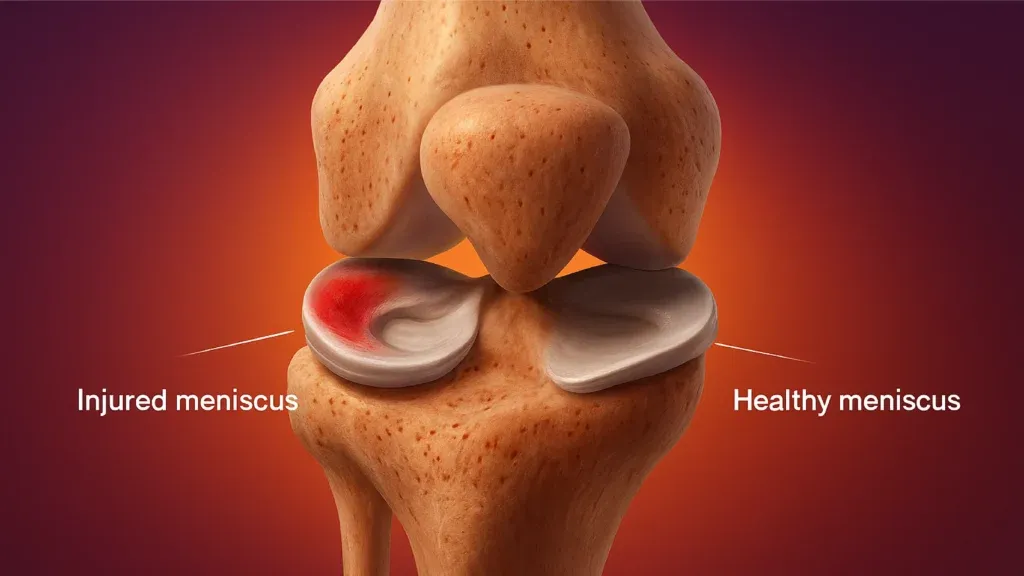
Hindistonda MCL va meniskusni ta'mirlash: jarrohlik, muvaffaqiyat darajasi va tiklanish

Rotator Cuff Repair Surgery in India: Procedure, Success Rates and Cost
Best Countries for Orthopaedic Surgery and Sports Medicine in 2026
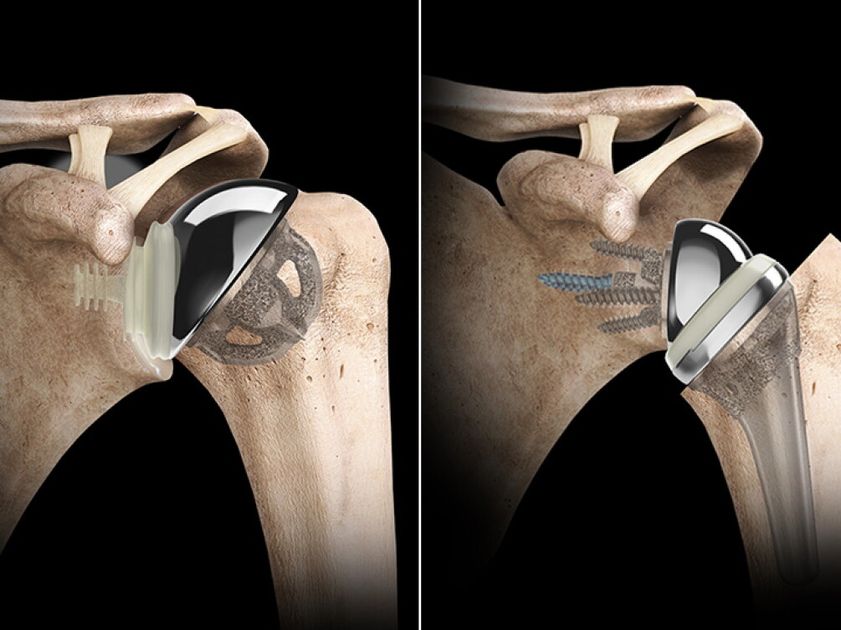
Hindistonda teskari elkani almashtirish: xarajat, protsedura, tiklanish

Hindistonda sonni qayta tiklash jarrohligi: protsedura, muvofiqlik va tiklanish

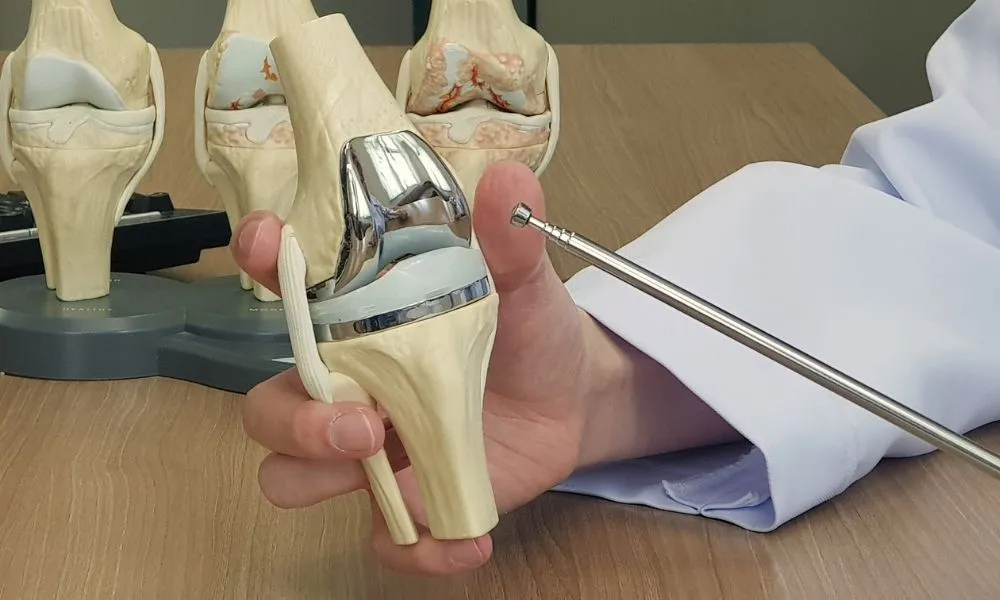
Hindistonda tizzani robot bilan almashtirish: foyda, natijalar va narx
Bizning veb-saytimiz cookie-fayllardan foydalanadi. Maxfiylik siyosati.