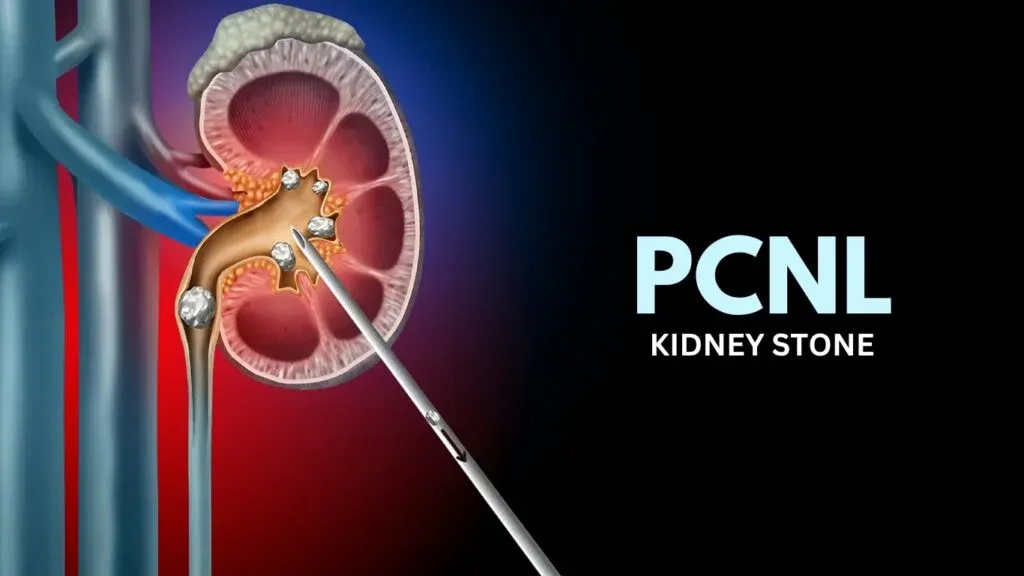
Энэтхэгт бөөрний том чулууг эмчлэх PCNL: журам, амжилтын хувь хэмжээ, өртөг
Холбоотой эмнэлэг
Энэхүү сэдэв нь чанарын эрүүл мэндийн үйлчилгээнд холбогдох эмнэлэг, эмнэлгийн төвүүд.

Medical Park Bahcelievler эмнэлэг
Medical Park Bahcelievler эмнэлэг нь Истанбул хотод 2007 онд байгуулагдсан, JCI байгууллагын магадлан итгэмжлэгдсэн 242 ортой эмнэлэг бөгөөд 33,000 ха...
Хэрцийлсэн

Нэгж

BLK-Max супер мэргэжлийн эмнэлэг, Нью Дели
Шинэ Дели дэх BLK-Max Super Specialty эмнэлэг нь 650 ортой, 22 дэвшилтэт мэс заслын тасаг, 13 мэргэжлийн төвийг санал болгодог Энэтхэгийн эрүүл мэндий...
Хэрцийлсэн

Нэгж

Fortis Memorial Research Institute (FMRI), Гургаон
Гургаон хотын Fortis Memorial Research Institute (FMRI) нь 2013 онд байгуулагдсан дэлхийн жишигт нийцсэн олон төрлийн мэргэжлийн эмнэлэг юм. Тус эмнэл...
Хэрцийлсэн
Нэгж

Артемис эмнэлэг, Гургаон
Гургаон хотын Артемис эмнэлэг нь 2007 онд байгуулагдсан JCI байгууллагын магадлан итгэмжлэгдсэн олон мэргэшлийн эмнэлэг бөгөөд 9 акр талбайд 750+ орто...
Хэрцийлсэн

Нэгж

Кокилабен Дирубхай Амбани эмнэлэг, Мумбай
Мумбай дахь Кокилабен Дирубхай Амбани эмнэлэг нь 2009 онд байгуулагдсан JCI, NABH, NABL, CAP-ийн магадлан итгэмжлэгдсэн дөрөв дэх шатлалын эмнэлэг юм....
Хэрцийлсэн
Нэгж

Медиковер эмнэлгүүд, Хайтек хот, Хайдарабад
Medicover Hospitals, Hitech City, Hyderabad нь 2011 онд байгуулагдсан 400 ортой NABH-ийн магадлан итгэмжлэгдсэн супер нарийн мэргэжлийн эмнэлэг юм. Эн...
Хэрцийлсэн
Нэгж
Холбоотой эмч нар
Энэ салбарт туршлагатай эмч, эмнэлгийн мэргэжилтнүүдтэй холбогдоорой.
Доктор Бибхас Ранжан Кунду
Ахлах зөвлөх
Доктор Ревати Р
Зөвлөх

Доктор Прасад Ражу Калидинди
Ахлах зөвлөх
Доктор Шакир Табрез
Нэмэлт захирал
Доктор Вичеан Камолпорнвижит
Зөвлөх

Доктор Укрид Кестхонг
Зөвлөх
Холбоотой хамаатгал
Эрүүл мэндийн ижил төстэй сэдвээр илүү олон нийтлэл, ойлголтыг судал.
Бөөрний чулууны эсрэг PCNL ба ESWL: аль нь илүү, хэзээ вэ?
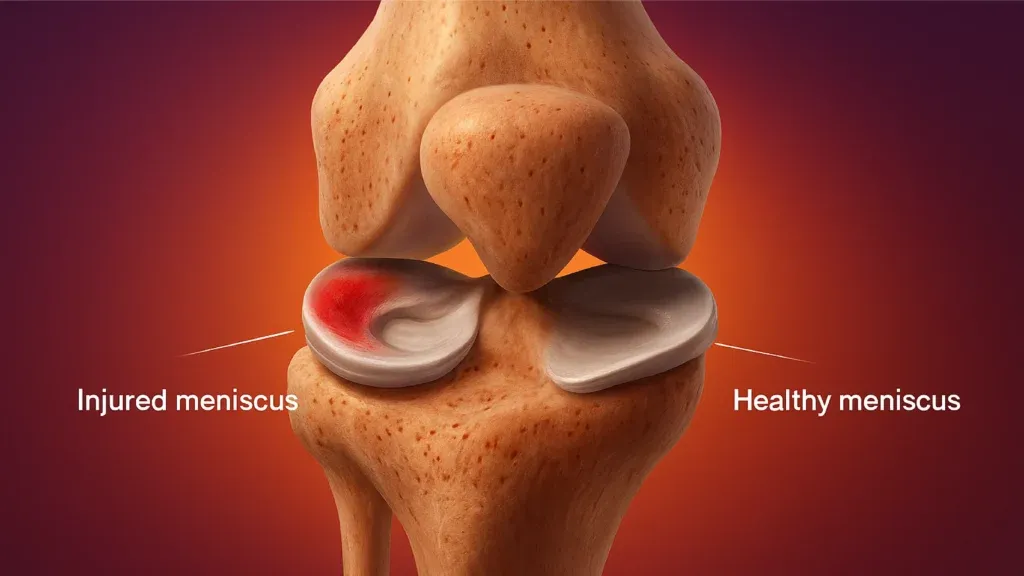
Энэтхэг дэх MCL ба менискийг засах: Мэс засал, амжилтын түвшин, нөхөн сэргээх

Rotator Cuff Repair Surgery in India: Procedure, Success Rates and Cost
Best Countries for Orthopaedic Surgery and Sports Medicine in 2026
Энэтхэг дэх ACL нөхөн сэргээх мэс засал: Процедур, өртөг, амжилтын түвшин
Энэтхэгт урвуу мөрөн солих: зардал, журам, нөхөн сэргээх
Манай вэбсайт нь жигнэмэг хэрэглэдэг. Нууцлалын бодлого.