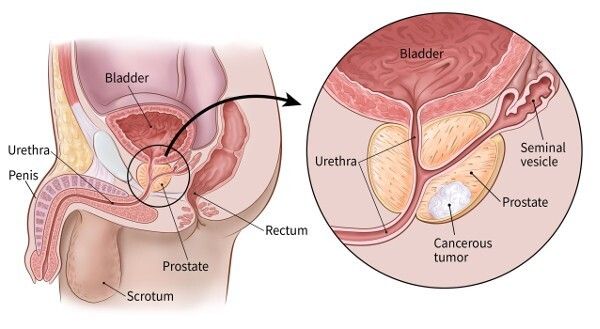
Robotic Prostatectomy in India: Nerve-Sparing Techniques, Recovery, and Patient Outcomes

Hospitali zinazohusiana
Gundua hospitali na vituo vya matibabu vinavyohusiana na mada hii kwa huduma bora za afya.

Hospitali ya Bahcelievler ya Hifadhi ya Matibabu
Hospitali ya Medical Park Bahcelievler ni hospitali iliyoidhinishwa na JCI ya vitanda 242 huko Istanbul, iliyoanzishwa mwaka wa 2007. Imeenea katika m...
Vibali

Vifaa

BLK-Max Super Specialty Hospital, New Delhi
BLK-Max Super Specialty Hospital huko New Delhi ni mojawapo ya taasisi kuu za afya ya India, inayotoa vitanda 650, kumbi 22 za upasuaji za hali ya juu...
Vibali

Vifaa

Taasisi ya Utafiti ya Fortis Memorial (FMRI), Gurgaon
Taasisi ya Utafiti ya Fortis Memorial (FMRI), Gurgaon, ni hospitali ya kiwango cha kimataifa ya wataalamu mbalimbali iliyoanzishwa mwaka wa 2013. Hosp...
Vibali
Vifaa

Hospitali ya Artemis, Gurgaon
Hospitali ya Artemis, Gurgaon, ni hospitali ya wataalamu wengi iliyoidhinishwa na JCI ambayo ilianzishwa mwaka wa 2007. Inatoa vitanda 750+ na miundom...
Vibali

Vifaa

Hospitali ya Kokilaben Dhirubhai Ambani, Mumbai
Hospitali ya Kokilaben Dhirubhai Ambani, Mumbai, ni JCI, NABH, NABL, na hospitali ya quaternary iliyoidhinishwa na CAP iliyoanzishwa mwaka wa 2009. Pa...
Vibali
Vifaa

Hospitali za Medicover, Hitech City, Hyderabad
Hospitali za Medicover, Hitech City, Hyderabad, ni hospitali ya utaalamu wa hali ya juu yenye vitanda 400 iliyoidhinishwa na NABH iliyoanzishwa mwaka ...
Vibali
Vifaa
Madaktari wanaohusiana
Ungana na madaktari wenye uzoefu na wataalamu wa matibabu katika uwanja huu.
Dk. Bibhas Ranjan Kundu
Mshauri Mkuu
Dkt. Revathi R
Mshauri

Dk. Prasad Raju Kalidindi
Mshauri Mkuu
Dk. Shakir Tabrez
Mkurugenzi wa ziada
Wichean Kamolpornvijit
Mshauri

Dk. Ukrid Kesthong
Mshauri
Nakala zinazohusiana
Chunguza nakala zaidi na ufahamu juu ya mada sawa za kiafya.
Matibabu ya HIFU kwa Saratani ya Prostate nchini India: Utaratibu, Gharama, na Uponaji

Laser Lithotripsy nchini India: Utaratibu, Teknolojia, Gharama na Urejeshaji

Je, Bima Yangu ya Matibabu ni halali nchini India? Mwongozo kwa Wagonjwa wa Kimataifa

India dhidi ya Thailand: Ni Eneo Lipi Bora la Utalii wa Matibabu mnamo 2026?
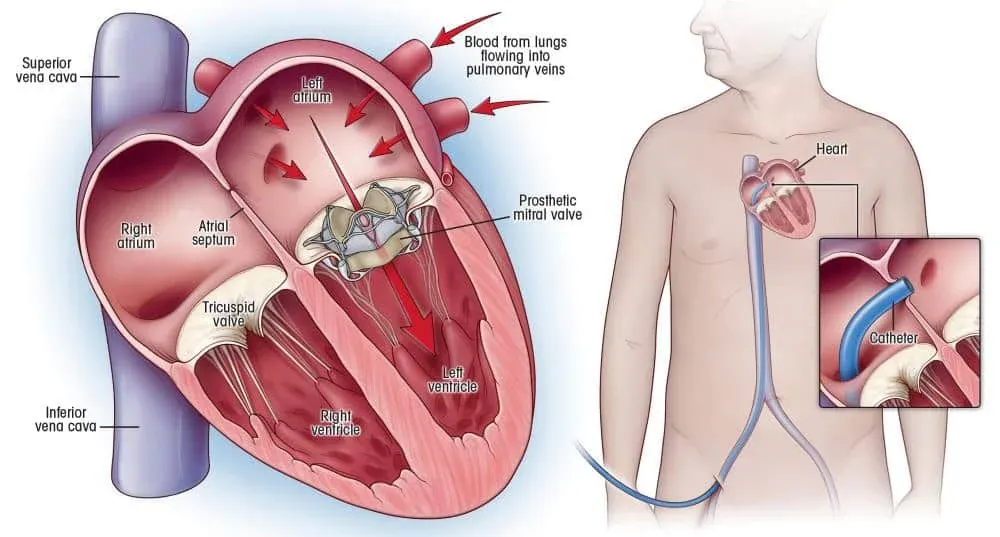
Heart Valve Replacement Surgery in India: Types, Technologies, and Recovery
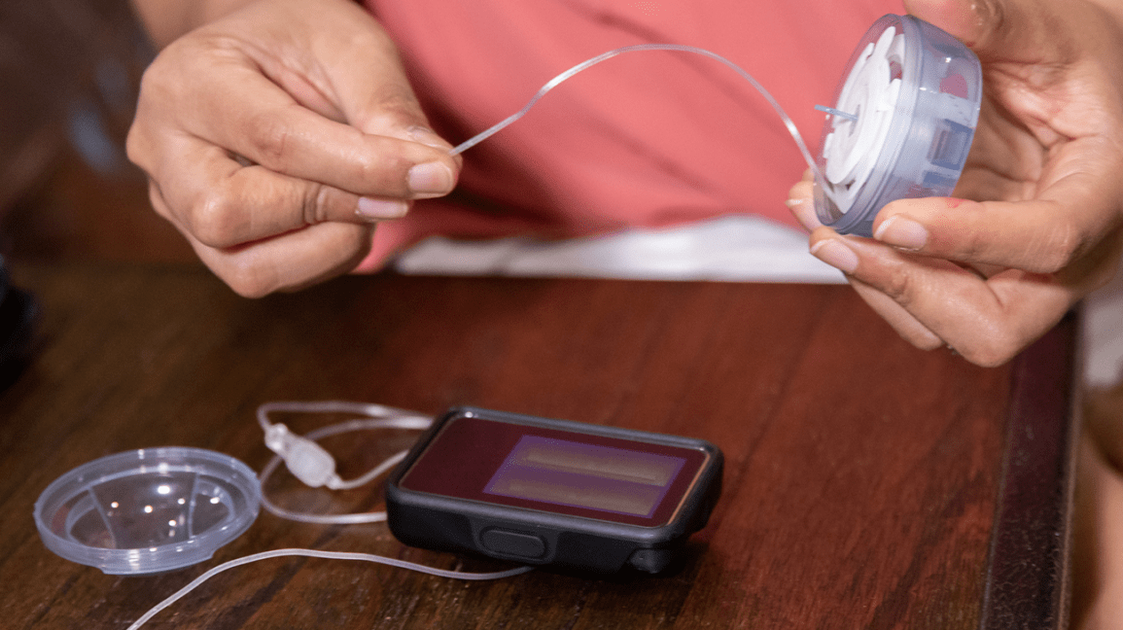
Tiba ya Pampu ya Insulini: Jinsi Inavyofanya Kazi, Nani Anafaidika, na Inagharimu Nini mnamo 2026

Tovuti yetu hutumia kuki. Sera ya faragha.