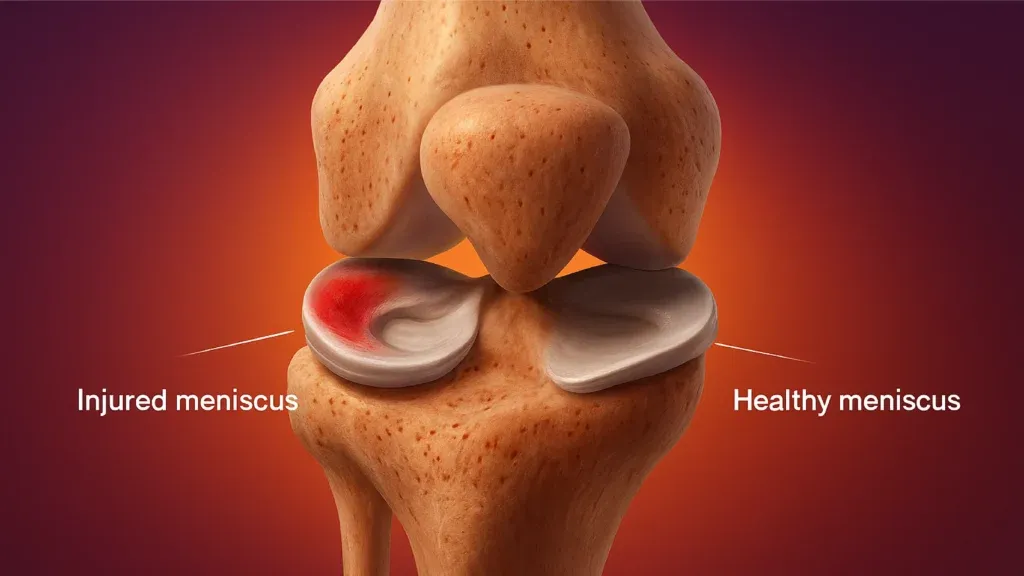
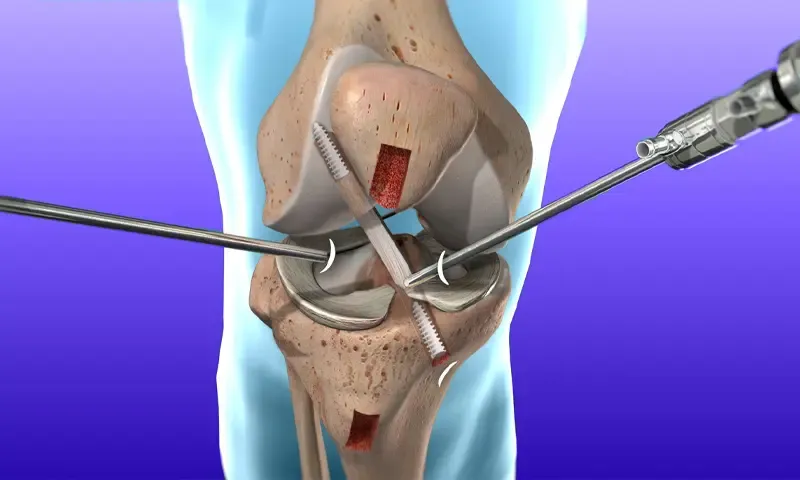
ការជួសជុល MCL និង Meniscus នៅក្នុងប្រទេសឥណ្ឌា៖ ការវះកាត់ អត្រាជោគជ័យ និងការស្តារឡើងវិញ
មន្ទីរពេទ្យពាក់ព័ន្ធ
ស្វែងរកមន្ទីរពេទ្យនិងមណ្ឌលសុខភាពទាក់ទងនឹងប្រធានបទនេះសម្រាប់សេវាកម្មថែទាំសុខភាពដែលមានគុណភាព។

ឧទ្យានវេជ្ជសាស្ត្រ Bahcelievler មន្ទីរពេទ្យ
Medical Park Bahcelievler Hospital គឺជាមន្ទីរពេទ្យដែលមានការទទួលស្គាល់ពី JCI ដែលមានគ្រែ 242 នៅទីក្រុងអ៊ីស្តង់ប៊ុល ដែលបានបង្កើតឡើងក្នុងឆ្នាំ 2007។ លាតសន...
ការទទួលស្គាល់

មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យឯកទេស BLK-Max ទីក្រុងញូវដេលី
មន្ទីរពេទ្យ BLK-Max Super Specialty Hospital នៅទីក្រុងញូវដេលី គឺជាស្ថាប័នថែទាំសុខភាពលំដាប់កំពូលមួយរបស់ប្រទេសឥណ្ឌា ដែលផ្តល់ជូននូវគ្រែចំនួន 650 រោងមហោស្...
ការទទួលស្គាល់

មធ្យោបាយបរិក្ខារ

វិទ្យាស្ថានស្រាវជ្រាវ Fortis Memorial (FMRI), Gurgaon
វិទ្យាស្ថានស្រាវជ្រាវ Fortis Memorial (FMRI) Gurgaon គឺជាមន្ទីរពេទ្យពហុឯកទេសលំដាប់ពិភពលោកដែលត្រូវបានបង្កើតឡើងក្នុងឆ្នាំ 2013។ មន្ទីរពេទ្យផ្តល់ជូនគ្រែច...
ការទទួលស្គាល់
មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យ Artemis, Gurgaon
មន្ទីរពេទ្យ Artemis, Gurgaon គឺជាមន្ទីរពេទ្យពហុឯកទេសដែលត្រូវបានទទួលស្គាល់ដោយ JCI ដែលត្រូវបានបង្កើតឡើងក្នុងឆ្នាំ 2007 ។ វាផ្តល់ជូននូវគ្រែចំនួន 750+ និង...
ការទទួលស្គាល់

មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យ Kokilaben Dhirubhai Ambani ទីក្រុងបុមបៃ
មន្ទីរពេទ្យ Kokilaben Dhirubhai Ambani ក្រុង Mumbai គឺជាមន្ទីរពេទ្យថែទាំសុខភាពប្រចាំត្រីមាសដែលត្រូវបានទទួលស្គាល់ដោយ JCI, NABH, NABL និង CAP ដែលបានបង្ក...
ការទទួលស្គាល់
មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យ Medicover, Hitech City, Hyderabad
មន្ទីរពេទ្យ Medicover, Hitech City, Hyderabad គឺជាមន្ទីរពេទ្យទំនើបពិសេសដែលទទួលស្គាល់ដោយ NABH ដែលមានគ្រែចំនួន 400 ដែលបានបង្កើតឡើងក្នុងឆ្នាំ 2011។ វាគឺជ...
ការទទួលស្គាល់
មធ្យោបាយបរិក្ខារ
គ្រូពេទ្យដែលពាក់ព័ន្ធ
ភ្ជាប់ទំនាក់ទំនងជាមួយវេជ្ជបណ្ឌិតដែលមានបទពិសោធន៍និងអ្នកឯកទេសខាងវេជ្ជសាស្ត្រក្នុងវិស័យនេះ។

បណ្ឌិត Kanchan Bhattacharyya
ទីប្រឹក្សា

Dr. Kalyan Guha
ទីប្រឹក្សា

Dr. Rajinder Singh Gaheer
ទីប្រឹក្សាជាន់ខ្ពស់

វេជ្ជបណ្ឌិត Ravi Bharadwaj
ទីប្រឹក្សាជាន់ខ្ពស់

វេជ្ជបណ្ឌិត Ranjan Kamilya
ទីប្រឹក្សាជាន់ខ្ពស់

លោកបណ្ឌិត Abheek Kar
ទីប្រឹក្សា
អត្ថបទពាក់ព័ន្ធ
ស្វែងរកអត្ថបទនិងការយល់ដឹងបន្ថែមលើប្រធានបទសុខភាពប្រហាក់ប្រហែល។

Rotator Cuff Repair Surgery in India: Procedure, Success Rates and Cost
Best Countries for Orthopaedic Surgery and Sports Medicine in 2026
ការវះកាត់កែទម្រង់ ACL នៅប្រទេសឥណ្ឌា៖ នីតិវិធី ការចំណាយ និងអត្រាជោគជ័យ
Reverse Shoulder Replacement in India: Cost, Procedure, Recovery

ការវះកាត់កែឆ្អឹងត្រគាកនៅប្រទេសឥណ្ឌា៖ នីតិវិធី សិទ្ធិទទួលបាន និងការស្តារឡើងវិញ

ការជំនួសជង្គង់មនុស្សយន្តនៅក្នុងប្រទេសឥណ្ឌា៖ អត្ថប្រយោជន៍ លទ្ធផល និងតម្លៃ
គេហទំព័ររបស់យើងប្រើខូឃីស៍។ គោលការណ៍ភាពឯកជន.