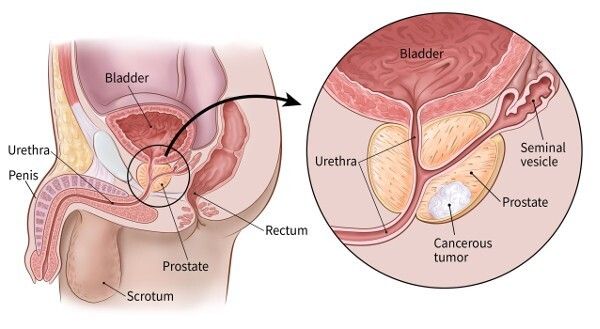
Robotic Prostatectomy in India: Nerve-Sparing Techniques, Recovery, and Patient Outcomes

មន្ទីរពេទ្យពាក់ព័ន្ធ
ស្វែងរកមន្ទីរពេទ្យនិងមណ្ឌលសុខភាពទាក់ទងនឹងប្រធានបទនេះសម្រាប់សេវាកម្មថែទាំសុខភាពដែលមានគុណភាព។

ឧទ្យានវេជ្ជសាស្ត្រ Bahcelievler មន្ទីរពេទ្យ
Medical Park Bahcelievler Hospital គឺជាមន្ទីរពេទ្យដែលមានការទទួលស្គាល់ពី JCI ដែលមានគ្រែ 242 នៅទីក្រុងអ៊ីស្តង់ប៊ុល ដែលបានបង្កើតឡើងក្នុងឆ្នាំ 2007។ លាតសន...
ការទទួលស្គាល់

មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យឯកទេស BLK-Max ទីក្រុងញូវដេលី
មន្ទីរពេទ្យ BLK-Max Super Specialty Hospital នៅទីក្រុងញូវដេលី គឺជាស្ថាប័នថែទាំសុខភាពលំដាប់កំពូលមួយរបស់ប្រទេសឥណ្ឌា ដែលផ្តល់ជូននូវគ្រែចំនួន 650 រោងមហោស្...
ការទទួលស្គាល់

មធ្យោបាយបរិក្ខារ

វិទ្យាស្ថានស្រាវជ្រាវ Fortis Memorial (FMRI), Gurgaon
វិទ្យាស្ថានស្រាវជ្រាវ Fortis Memorial (FMRI) Gurgaon គឺជាមន្ទីរពេទ្យពហុឯកទេសលំដាប់ពិភពលោកដែលត្រូវបានបង្កើតឡើងក្នុងឆ្នាំ 2013។ មន្ទីរពេទ្យផ្តល់ជូនគ្រែច...
ការទទួលស្គាល់
មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យ Artemis, Gurgaon
មន្ទីរពេទ្យ Artemis, Gurgaon គឺជាមន្ទីរពេទ្យពហុឯកទេសដែលត្រូវបានទទួលស្គាល់ដោយ JCI ដែលត្រូវបានបង្កើតឡើងក្នុងឆ្នាំ 2007 ។ វាផ្តល់ជូននូវគ្រែចំនួន 750+ និង...
ការទទួលស្គាល់

មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យ Kokilaben Dhirubhai Ambani ទីក្រុងបុមបៃ
មន្ទីរពេទ្យ Kokilaben Dhirubhai Ambani ក្រុង Mumbai គឺជាមន្ទីរពេទ្យថែទាំសុខភាពប្រចាំត្រីមាសដែលត្រូវបានទទួលស្គាល់ដោយ JCI, NABH, NABL និង CAP ដែលបានបង្ក...
ការទទួលស្គាល់
មធ្យោបាយបរិក្ខារ

មន្ទីរពេទ្យ Medicover, Hitech City, Hyderabad
មន្ទីរពេទ្យ Medicover, Hitech City, Hyderabad គឺជាមន្ទីរពេទ្យទំនើបពិសេសដែលទទួលស្គាល់ដោយ NABH ដែលមានគ្រែចំនួន 400 ដែលបានបង្កើតឡើងក្នុងឆ្នាំ 2011។ វាគឺជ...
ការទទួលស្គាល់
មធ្យោបាយបរិក្ខារ
គ្រូពេទ្យដែលពាក់ព័ន្ធ
ភ្ជាប់ទំនាក់ទំនងជាមួយវេជ្ជបណ្ឌិតដែលមានបទពិសោធន៍និងអ្នកឯកទេសខាងវេជ្ជសាស្ត្រក្នុងវិស័យនេះ។
បណ្ឌិត Bibhas Ranjan Kundu
ទីប្រឹក្សាជាន់ខ្ពស់
បណ្ឌិត រ៉េវ៉ាធី អរ
ទីប្រឹក្សា

បណ្ឌិត Prasad Raju Kalidindi
ទីប្រឹក្សាជាន់ខ្ពស់
វេជ្ជបណ្ឌិត Shakir Tabrez
នាយកបន្ថែម
បណ្ឌិត Wichean Kamolpornvijit
ទីប្រឹក្សា

បណ្ឌិត Ukrid Kesthong
ទីប្រឹក្សា
អត្ថបទពាក់ព័ន្ធ
ស្វែងរកអត្ថបទនិងការយល់ដឹងបន្ថែមលើប្រធានបទសុខភាពប្រហាក់ប្រហែល។
ការព្យាបាល HIFU សម្រាប់ជំងឺមហារីកក្រពេញនៅក្នុងប្រទេសឥណ្ឌា៖ នីតិវិធី ការចំណាយ និងការស្តារឡើងវិញ

ឡាស៊ែរ Lithotripsy នៅប្រទេសឥណ្ឌា៖ នីតិវិធី បច្ចេកវិទ្យា ការចំណាយ និងការស្តារឡើងវិញ

តើការធានារ៉ាប់រងវេជ្ជសាស្រ្តរបស់ខ្ញុំមានសុពលភាពនៅក្នុងប្រទេសឥណ្ឌាដែរឬទេ? មគ្គុទ្ទេសក៍សម្រាប់អ្នកជំងឺអន្តរជាតិ

India vs Thailand: Which is the Best Medical Tourism Destination in 2026?
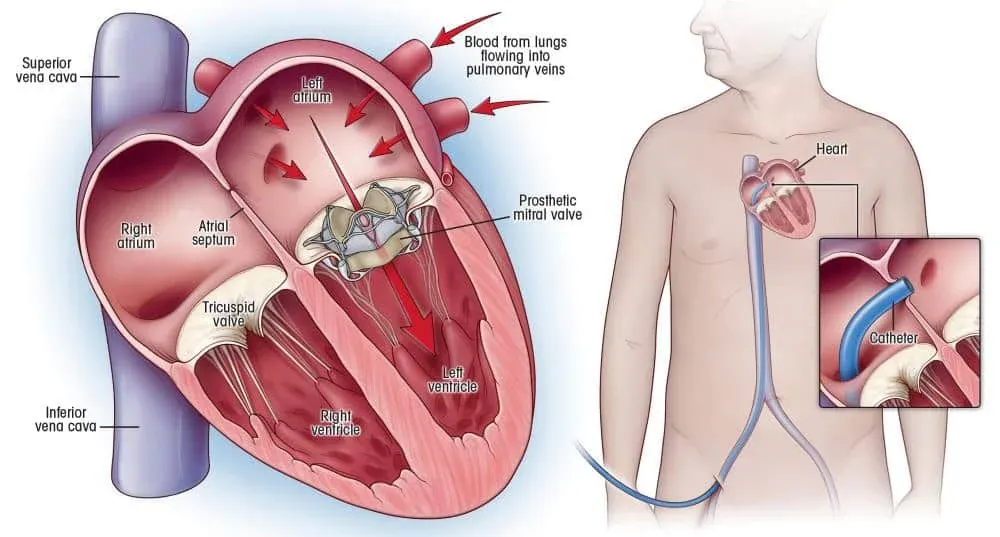
ការវះកាត់ប្តូរវ៉ាល់បេះដូងនៅប្រទេសឥណ្ឌា៖ ប្រភេទ បច្ចេកវិទ្យា និងការស្តារឡើងវិញ
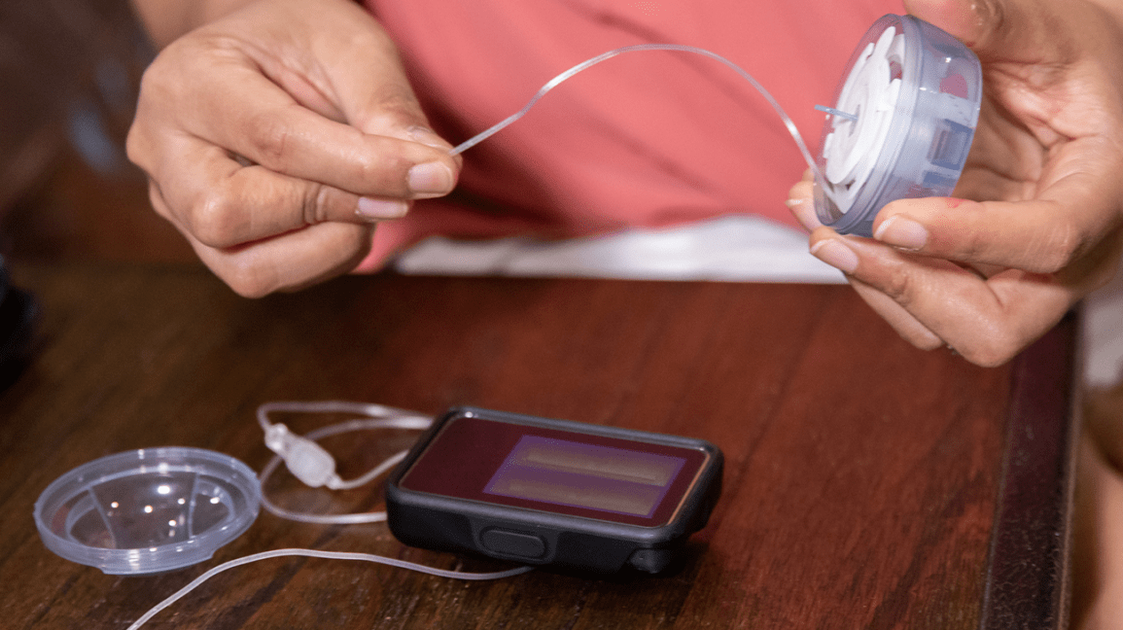
ការព្យាបាលដោយបូមអាំងស៊ុយលីន៖ របៀបដែលវាដំណើរការ តើអ្នកណាទទួលបានអត្ថប្រយោជន៍ និងអ្វីដែលវាចំណាយក្នុងឆ្នាំ 2026

គេហទំព័ររបស់យើងប្រើខូឃីស៍។ គោលការណ៍ភាពឯកជន.